Rohit S. Loomba
DOI: 10.13140/RG.2.2.18686.50246
The International Pediatric and Congenital Cardiac Code (IPCCC) and the upcoming International Classification of Disease-11 (ICD-11) define a cleft mitral valve as “A congenital cardiac malformation of the mitral valve in which the anterior leaflet is divided into two parts”. As a member of the International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD), I have myself participated in the discussions surrounding the creation of the ICD-11 codes and their definitions. The group ,as a whole, consists of individuals from across the world. It has representatives from those who ascribe to a variety of cardiac anatomic schools of thought and thus reflects many views.
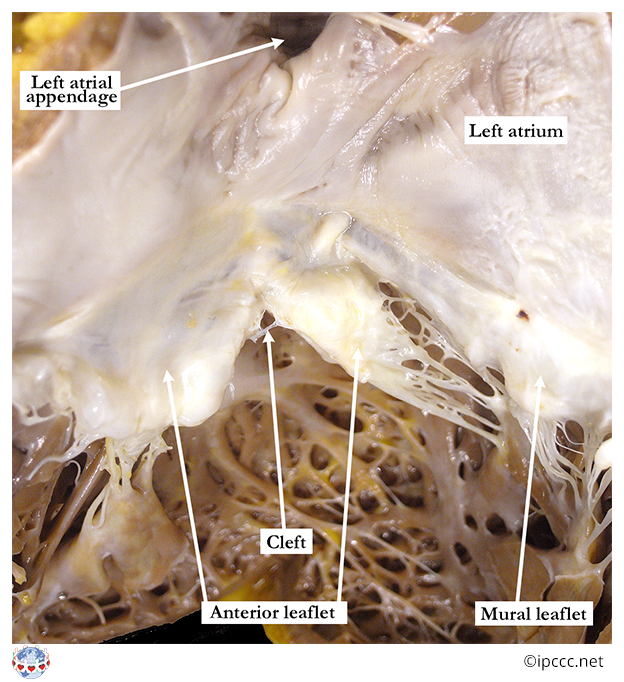
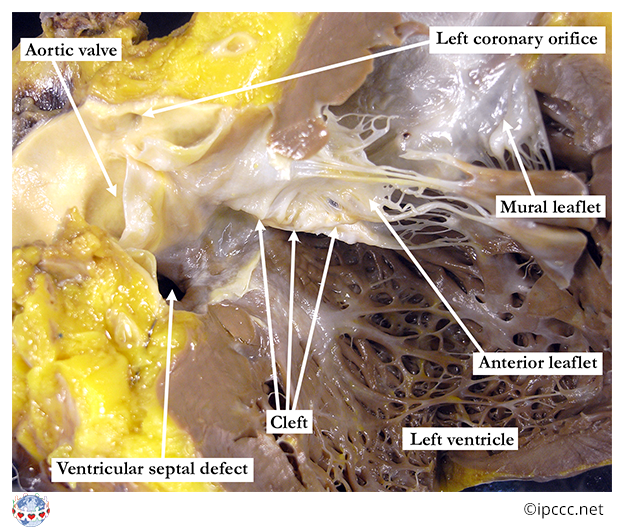
The image above consists of a heart specimen with the mitral valve exposed. The specimen is exposed such that the anterior surface is coming out wards the screen and the posterior surface is into the screen. Superior is towards the top of the screen and inferior is towards the bottom of the screen. Specimen left is towards the right of the image and specimen right is towards the left of the image. The anterior leaflet is seen here and there is a “tear” in the anterior leaflet that divides into portions. This is a cleft and points towards the aortic outflow tract. This notion of the directionality of a cleft was first posited by Becker and colleagues and then subsequently demonstrated in clinical studies.
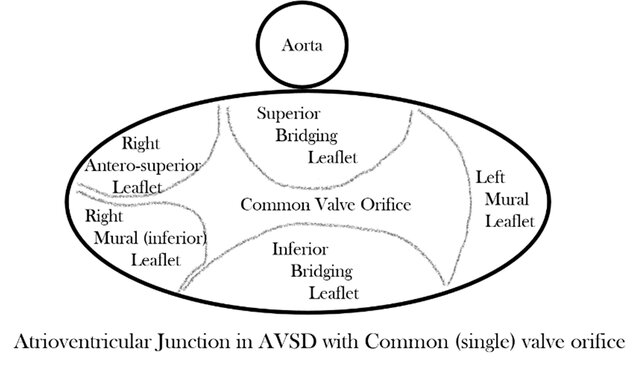
This definition is important, particularly in the context of an atrioventricular septal defect. In the setting of an atrioventricular septal defect there is a common atrioventricular junction with left and right fibrous valvar components. The common atrioventricular valve has five major components: the superior bridging leaflet, the inferior bridging leaflet, the antero-superior leaflet, the right mural leaflet, and the left mural leaflet. The superior bridging leaflet will often have a distinct right and left component.
The surgical repair of this lesion includes dividing this valve into a right and left atrioventricular valve as well as closing any atrial or ventricular level shunts. These must be done with care taken to ensure that the resulting right- and left-sided atrioventricular valves do not have significant stenosis or regurgitation. Often, the surgical repair will consist of “closing a cleft”.
But what is the so-called “cleft” of the left atrioventricular valve in the setting of an atrioventricular septal defect? The figure below demonstrates what many refer to as the alleged “cleft”. It is the leftward component of the zone of apposition (where two valve leaflets come together or appose when closed) between the superior and bridging leaflet. It is not a deficiency in a single leaflet itself, it is simply where the two valve leaflets coapt. We certainly do not refer to deficiencies in copatiation as “clefts” for other valves.
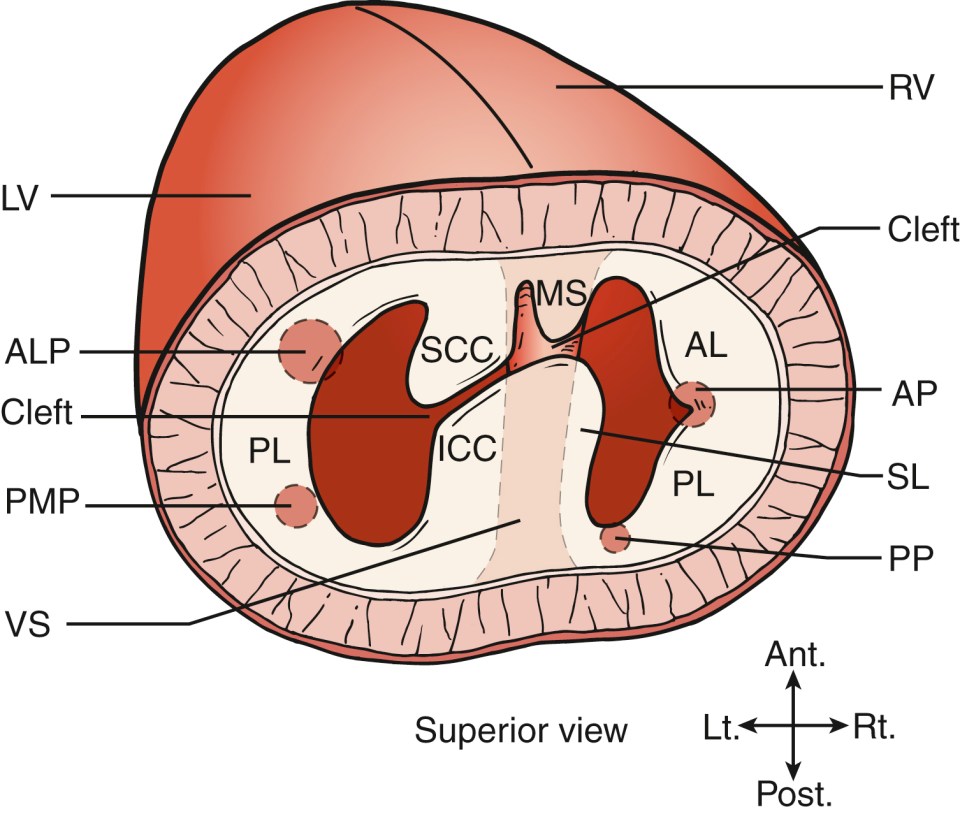
Carpentier and colleagues described the left-sided component of the common atrioventricular valve in the setting of atrioventricular septal defect with respect to its management in 1978. This paper rightfully identified that the so-called “cleft” was actually a commisure or zone of apposition. They supported this statement by highlighting the findings that the so-called “cleft” was not supported by commisural chords or papillary muscles, analogous to the gaps between the arterial valve leaflets that have been described as commisures or zones of apposition as they are not supported by chords or papillary muscles.
Work by Ugarte and colleagues as well as Piccoli and colleagues subsequently endorsed this notion put forth by Carpentier and colleagues that the gap being referred to as the “cleft” by some is actually a the left-sded component of the commisure or zone of apposition between the superior and inferior bridging leaflets.
Some will approach this with a “who cares”, but if the purpose of language is to communicate ideas and knowledge effectively we must make sure our descriptions of phenomena are in concordance with this. If we are to assume that language is acceptable if there are community-based exceptions to how words are used then this could lead to misunderstanding of the underlying meaning of words between groups who assign a different community-based definition. This would obviously pose a large linguistic obstacle as well.
With respect to the left-sided atrioventricular valve and the so-called “cleft”, if we accept this inaccuracy in labeling then it would be fair for all commisures with some regurgitation to be referred to as “clefts”. This certainly would not be helpful with communication regarding valvar structure and would lead to much confusion.
Click on the image below for more specimen-image based cardiac anatomy education/review!


